What is kidney cancer?
Kidney cancer starts in the cells of the kidney. Cancerous (malignant) tumor is a group of cancer cells that can invade and destroy nearby tissue. The tumor can also spread (metastasize) to other parts of the body.
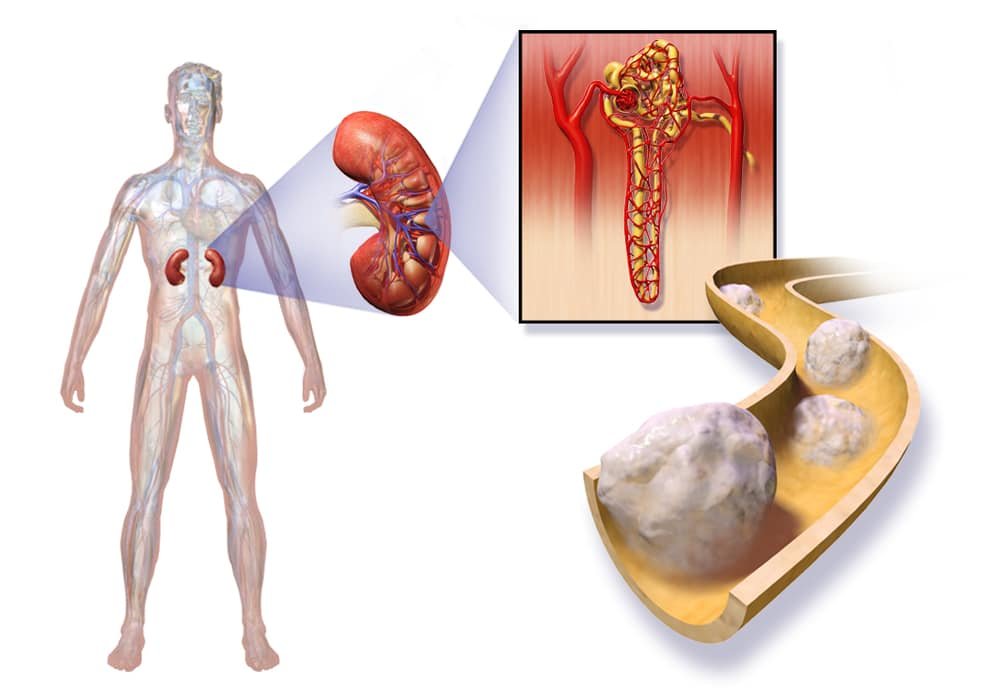
The kidneys are part of the urinary tract. We have two kidneys, one on each side of the spine, deep in the upper abdomen. The kidneys are part of the urinary tract. The body contains 2 kidneys, one on either side of the spine below the lower ribs, deep in the upper abdomen. The ureters are thin tubes that connect each kidney to the bladder. They are about 25 to 30 cm (10 to 12 inches) long. The urethra is a small tube that connects the bladder to the outside of the body. There is an adrenal gland just above each kidney. The adrenal glands are part of the endocrine system.
An adrenal gland sits above each kidney. The kidneys make urine by filtering water and waste products from the blood. Inside each kidney is a network of millions of tiny tubes called nephrons. Each nephron is made up of a tubule and a corpuscle. Tubules are tiny tubes that collect wastes and chemicals. The corpuscles contain a collection of very small blood vessels that filter blood.
Kidney cells sometimes undergo changes that make the way they grow or behave abnormally. These changes can lead to the development of non-cancerous (benign) conditions such as cysts. They can also cause non-cancerous tumors such as papillary adenoma of the kidney to form.
But in some cases, changes in kidney cells can cause kidney cancer. Most of the time, kidney cancer starts in the cells that line the tubules. This type of cancer is called classic renal cell carcinoma, or clear cell carcinoma. Cancers that start in other cells of the kidney are called non-clear cell carcinomas.
Rare types of kidney cancer can also occur. Examples are renal sarcoma and primary renal lymphoma.
Kidney function
The main function of the kidneys is to filter water, impurities and waste products from the blood.
Blood enters the kidneys through the renal arteries. Once in the kidneys, the blood passes through the nephrons, where waste products and excess water are drained. The purified blood returns to the body through the renal veins.
The filtered wastes from the blood are then concentrated to form urine. The urine is collected by the pelvis. The ureters carry urine into the bladder, where it is stored. Urine is then passed from the bladder and then out of the body through the urethra.
The kidneys also act as endocrine glands. They produce these hormones:
- erythropoietin (EPO), which causes the bone marrow to make red blood cells
- calcitriol, a form of vitamin D, which helps the colon absorb calcium from food
- renin, which helps regulate blood pressure
Cancerous tumors of the kidney
The cancerous tumor of the kidney can invade and destroy nearby tissue. It can also spread (metastasize) to other parts of the body. Cancerous tumor is also called a malignant tumor. Different types of cancerous tumors can appear in different parts of the kidney.
Renal cell carcinoma
Renal cell carcinoma (RCC) is the most common type of kidney cancer. It originates in the lining of the tubules of the kidney.
Types of CCR
There are several types of CCRs, including the following.
Clear cell carcinoma is the most common type of CRC. About 80% of all CRCs are clear cell carcinomas. Under the microscope, the cancer cells present in these tumors are very pale or clear.
Papillary carcinoma is the second most common type of CRC. The cancer cells in this tumor are shaped like little fingers. Papillary carcinoma of the kidney is divided into 2 types. Type 1 is a low-grade tumor that does not spread very quickly. Type 2 is a high grade tumor that can spread quickly.
Chromophobic carcinoma is made up of large, pale brown cancer cells that often look like a cobblestone street. Chromophobic carcinoma has a better prognosis than other types of kidney cancer.
Unclassifiable CRCs are tumors that do not fit into any other category of CRC. Cancer cells look different from any other type of CRC.
Rare kidney tumors
The following cancerous tumors of the kidney are rare:
- collector tube carcinoma
- medullary carcinoma
- multilocular cystic carcinoma
Other rare kidney tumors
Here are other rare cancerous tumors of the kidney.
Cancer of the renal pelvis starts in the cells that line the renal pelvis, ureters and bladder. The type of cancer that appears in these cells is called urothelial, or transitional, carcinoma.
Kidney sarcoma starts in the connective tissues or blood vessels of the kidney. There are different types of kidney sarcomas, including leiomyosarcoma, angiosarcoma, and rhabdomyosarcoma.
Primary renal lymphoma is a very rare tumor with a poor prognosis. The most common type is diffuse large B cell lymphoma (LDGCB).
Wilms tumor is a type of kidney cancer that is usually diagnosed in children. It very rarely affects adults.
Tumors and non-cancerous conditions of the kidney
A non-cancerous (benign) kidney tumor is a lump that does not spread to other parts of the body (not metastasize). The non-cancerous tumor is usually not life threatening. It is usually removed by surgery and usually does not come back (come back).
Non-cancerous kidney disease is a change in the cells of the kidney, but it is not cancer. The non-cancerous condition does not spread to other parts of the body and is usually not life threatening.
There are various types of kidney tumors and non-cancerous conditions.
Non-cancerous tumors
Papillary adenoma
Papillary adenoma is the most common non-cancerous tumor of the kidney. It is a small, slowly growing lump that usually doesn’t cause symptoms. It is often detected on an imaging test done for other reasons.
Oncocytoma
The oncocytoma starts in the cells of the kidney’s collecting tubes. This tumor can get quite large. Several oncocytomas can be seen in a single kidney or in both. It can be detected at the same time as a cancerous tumor.
Angiomyolipoma
Angiomyolipoma is a kidney tumor made up of fat, blood vessels, and smooth muscle tissue. It often occurs in people with tuberous sclerosis, a genetic disorder that causes non-cancerous tumors to form in many organs, including the eyes, skin, brain, lungs, heart, and kidneys. Even though it is non-cancerous, this tumor can spread to nearby tissue and destroy it. A tumor that is more than 4 cm (1 ½ inch) in diameter can also cause sudden bleeding (hemorrhage) from the kidney into the abdomen.
Treatments
Surgery is the main treatment for non-cancerous kidney tumors. Here are other treatment options:
- active surveillance
- arterial embolization (for angiomyolipoma)
Non-cancerous conditions
A simple cyst is the most common non-cancerous kidney disease. The simple cyst is a round or oval sac filled with fluid. One or more cysts may appear in the kidney. Simple kidney cyst is very common in people over the age of 50.
Most simple kidney cysts are found on imaging tests for other medical reasons. When seen on imaging, simple kidney cysts have rounded, smooth, and well-defined contours. This helps doctors differentiate them from kidney tumors.
If the simple kidney cyst is not causing any symptoms, it does not need to be treated. If it starts to cause problems (pain, infection, or bleeding, for example), the doctor will drain the cyst with a long needle or have it removed by surgery.
Active Cancer Surveillance and Visits | Monitoring and Follow-up for Cancer Survivors
Risk factors for kidney cancer
A risk factor is something, like a behavior, substance, or condition that increases your risk for developing cancer. Most cancers are caused by many risk factors, but kidney cancer can develop in people who do not have any of the risk factors described below.
Kidney cancer most often affects people over the age of 50. It is observed more in men than in women.
Risk factors are usually ranked from most important to least important. But in most cases, it is impossible to rank them with absolute certainty.
Risk factors
Smoking tobacco
Overweight and obesity
High blood pressure
Certain inherited genetic disorders
End-stage renal disease and dialysis
Family history of kidney cancer
Contact with trichlorethylene at work
Tall adult height
There is convincing evidence that the following factors increase your risk for kidney cancer.
Smoking tobacco
Your risk of developing kidney cancer increases depending on the amount of tobacco you smoke and the length of time you smoke.
Overweight and obesity
Being overweight and obese increases the risk of kidney cell carcinoma (RCC), the most common type of kidney cancer. Researchers are trying to find out how overweight and obesity increase the risk of kidney cancer.
High blood pressure
It is not known exactly how high blood pressure increases the risk of kidney cancer.
Certain inherited genetic disorders
The following hereditary genetic disorders increase the risk of different types of kidney cancer tumors. People with one of these inherited genetic disorders get kidney cancer at a younger age than other people. These inherited genetic disorders are not very common and cause only a small number of all kidney cancers.
Von Hippel-Lindau disease (VHL) is a rare inherited condition characterized by the formation of tumors and cysts in different parts of the body, including the kidneys. Tumors usually appear in young adults. VHL disease increases the risk of clear cell carcinoma of the kidney.
Hereditary renal papillary cell carcinoma (HPRC) is an inherited form of kidney cancer characterized by the development of multiple papillary carcinomas in both kidneys. It is also called papillary renal cell carcinoma type 1.
Hereditary leiomyomatosis and renal cell carcinoma (HLRCC) increases the risk of developing non-cancerous tumors, called leiomyomas, in the skin or uterus. It also increases the risk of papillary renal cell carcinoma type 2.
Birt-Hogg-Dubé syndrome (BHD) is a very rare genetic disorder that affects the skin and lungs. It also increases the risk of certain types of tumors, including cancerous and non-cancerous kidney tumors. People with BHD syndrome can have different types of kidney cancer, such as chromophobic carcinoma and clear cell carcinoma.
Tuberous sclerosis (TS) can cause non-cancerous tumors to form in many organs including the eyes, skin, brain, lungs, heart and kidneys. People with TS are at increased risk for kidney cysts and kidney cancer, including angiomyolipoma (a non-cancerous tumor of the kidney), chromophobic carcinoma and clear cell carcinoma.
End-stage renal disease and dialysis
End-stage kidney disease occurs when the kidneys are no longer able to remove waste products from the blood, which is why a person needs a kidney transplant or dialysis. Dialysis is a process that takes the place of the kidneys to remove waste products from the blood.
Cysts can appear in the kidneys of people on dialysis for a long time (acquired cystic kidney disease). Acquired cystic kidney disease increases the risk of kidney cancer. The risk of kidney cancer seems to increase the longer you take dialysis.
People who have had a kidney transplant also seem to be at greater risk of developing kidney cancer in the other kidney, which is the kidney that was not transplanted.
Family history of kidney cancer
People with a first-degree relative (father, mother, brother, sister or child) who have kidney cancer are more likely to have the disease themselves. The risk is greater if the parent is a sibling.
Contact with trichlorethylene at work
Trichlorethylene (TCE) is an industrial solvent used mainly in metal degreasing. People who come in contact with TCE at work are more likely to develop kidney cancer. This risk increases the higher the level of exposure.
Tall adult height
Research shows that the taller a person, the higher their risk of developing kidney cancer. It is not clear exactly why being tall increases the risk.
Possible risk factors
The following factors have been linked to kidney cancer in some way, but there is not enough evidence to say that they are risk factors. More research is needed to clarify the role of these factors in the development of kidney cancer:
- contact with welding fumes or cadmium at work
- horseshoe kidney (rare birth defect where the tissue that forms the kidneys does not separate to form 2 separate kidneys)
- arsenic in drinking water
- personal history of thyroid cancer
- hysterectomy
- radiation exposure
- hepatitis C infection
No link to kidney cancer
Important evidence does not show a link between kidney cancer and drinking coffee or tea. There is also evidence that drinking alcohol (up to 2 drinks per day) reduces the risk of kidney cancer. However, it is important to remember that there is strong evidence that alcohol consumption increases the risk of developing several other cancers. Therefore, alcohol should not be drunk to reduce the risk of developing kidney cancer.
Reducing your risk for kidney cancer
You may lower your risk of developing kidney cancer by doing the following.
Live smoke-free
Smoking tobacco increases the risk for kidney cancer. If you smoke, get help to quit smoking.
Have a healthy body weight
Research shows that overweight and obesity increases your risk for kidney cancer. You can lower your risk by having a healthy body weight. Eating well and being physically active can help you have a healthy body weight.
Keep high blood pressure under control
If you have high blood pressure, talk to your healthcare team about ways you can keep it under control.
Follow health and safety guidelines at work
Coming into contact with trichlorethylene (TCE) increases your risk for kidney cancer. Having contact with cadmium and welding fumes may also put you at risk. Following health and safety guidelines can help you lower your contact with these chemicals at work.
Finding kidney cancer early
When kidney cancer is found and treated early, the chances of successful treatment are better. Get regular health checkups and see your doctor if you have any symptoms or are worried about your health.
If you have a higher than average risk, you may need to visit your doctor more often to check for kidney cancer. Talk to your doctor about tests that can help find kidney cancer early, including the following:
- ultrasound
- CT scan
Symptoms of kidney cancer
Kidney cancer may not cause any signs or symptoms in the very early stages of the disease. It is usually detected on an ultrasound or an x-ray done for some other reason. Signs and symptoms often appear as the tumor grows in nearby tissues and organs. Other medical conditions can cause the same symptoms as kidney cancer.
See your doctor if you have the following signs or symptoms:
- blood in urine (hematuria) (most common)
- pain in the back and side of the abdomen
- mass that can be felt in the abdomen
- swelling of the legs and ankles
- high blood pressure
- low number of red blood cells (anemia)
- tired
- night sweats
- weightloss
- loss of appetite
- fever
- in men, large swollen vein in the scrotum (varicocele)
Kidney cancer diagnosis
Diagnosis is a process of identifying the cause of a health problem. The diagnostic process for kidney cancer usually begins with a visit to your family doctor. Your doctor will ask you about your symptoms and do a physical exam. Based on this information, your doctor will refer you to a specialist or order tests to check for kidney cancer or other health problems.
The diagnostic process can seem long and overwhelming. It’s okay to worry, but try to remember that other medical conditions can cause symptoms similar to kidney cancer. It is important that the healthcare team rule out any other possible cause of the condition before making a diagnosis of kidney cancer.
The following tests are usually used to rule out or diagnose kidney cancer. Many tests that can diagnose cancer are also used to determine the stage, that is, how far the disease has spread. Your doctor may also give you other tests to check your general health and to help plan your treatment.
Health history and physical examination
Your health history consists of a checkup of your symptoms, your risks, and any medical events and conditions you may have had in the past. Your doctor will ask you questions about your history:
- symptoms that suggest kidney cancer
- smoking
- high blood pressure
- overweight and obesity
Your doctor may also ask you questions about your family history:
- kidney cancer
- risk of kidney cancer
- other cancers
The physical exam allows your doctor to look for any signs of kidney cancer. During the physical exam, your doctor may feel your abdomen, back, and sides to see if there is a lump in the kidney area.
Urine analysis
A urinalysis is a test that measures substances such as electrolytes, hormones and blood in the urine. If there is blood in the urine, it means there is bleeding in the kidneys or urinary tract.
Blood biochemical analyzes
A blood chemistry test measures the level of chemicals in the blood. It makes it possible to assess the quality of functioning of certain organs and also to detect anomalies. Blood chemistry tests that are used to diagnose kidney cancer include these.
Blood urea nitrogen and creatinine levels can be measured to find out how well the kidneys are functioning. If the levels are high, it could mean that the kidneys are not working well, possibly because of cancer.
Glomerular filtration rate (GFR) is another test that shows how well the kidneys are functioning. The amount of blood that passes through the glomeruli, the tiny filters in the kidneys that remove waste products from the blood, is assessed. The level of creatinine in the blood is measured and calculated by combining it with several other factors, including age, sex, height, weight and ethnicity, to establish the GFR. A low GFR means that the kidneys are not filtering the blood very well and could suggest a kidney problem.
Calcium and phosphorus levels may be high if you have kidney disease or if the cancer has spread to your bones.
The level of alkaline phosphatase may be high if the kidney cancer has spread to the bones or the liver.
Liver function tests can be done to find out if there is a problem with the liver.
Complete blood count
The complete blood count (CBC) is used to assess the quantity and quality of white blood cells, red blood cells and platelets. FSC is used to check for anemia (low red blood cell count) caused by bleeding that has lasted for a long time. Anemia very often affects people with kidney cancer.
In very rare cases, kidney cancer can produce a hormone called erythropoietin. This hormone causes the bone marrow to make too many red blood cells. The CBC results will tell your doctor if your red blood cell count is higher than normal.
FSC is also used to make sure the person is healthy enough to have surgery.
CT scan
In a computed tomography (CT), special x-ray machines are used to produce 3-dimensional images and in sections of the organs, tissues, bones and blood vessels of the body. A computer assembles the photos into detailed images.
CT is the most common imaging test used to diagnose kidney cancer. It provides information about the size, shape and location of the tumor. It also helps to know if the tumor has spread to the lymph nodes, blood vessels or other organs.
CT can also help guide the doctor to the tumor during a biopsy.
Ultrasound
In an ultrasound, high-frequency sound waves are used to produce images of parts of the body. It helps to look for changes in the kidneys. It can tell the difference between a cyst, which contains fluid, and a solid tumor.
The ultrasound can also help guide the doctor to the tumor during a biopsy.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) uses powerful magnetic forces and radio waves to produce cross-sectional images of the body’s organs, tissues, bones, and blood vessels. A computer assembles the images into 3-dimensional snapshots.
Sometimes an MRI is done to check if the cancer has spread to the main blood vessels in the kidney or to other organs.
An MRI is not used if the results of CT and other imaging tests clearly show the tumor to the kidney and how far it has spread.
Biopsy
During the biopsy, the doctor removes tissues or cells from the body for analysis in the laboratory. The pathologist’s report confirms whether or not there are cancer cells in the sample.
A kidney biopsy is not usually done to diagnose kidney cancer. Imaging tests such as CT and ultrasound can usually confirm the diagnosis.
In some cases, a biopsy may be taken to remove some tissue from an area that may be cancerous if the imaging tests have not been clear enough to make a diagnosis. A biopsy may be taken before treatment if the tumor is small and the person is not well enough to have surgery.
Angiography
Angiography uses pictures to show how blood is flowing through the blood vessels in the kidneys, which helps plan treatment.
X-ray
In an x-ray, low-dose radiation is used to produce images of parts of the body on film. A chest x-ray is done to see if the kidney cancer has spread to the lungs.
Bone scan
In a bone scan, radioactive materials that attach to the bones (radiopharmaceuticals) and a computer are used to create an image of the bones. It is used to find out if kidney cancer has spread to the bones. A bone scan is usually done if blood chemistry tests, such as an increase in alkaline phosphatase or calcium levels, suggest that kidney cancer has spread to the bones.
Kidney cancer grades
The grade, or histological classification, defines how cancerous cells look when compared to normal, healthy cells. Knowing the grade gives your healthcare team an idea of how quickly cancer can grow and how likely it is to spread. It helps him plan your treatment. The grade can also help the healthcare team determine the possible outcome of the disease (prognosis) and predict how the cancer might respond to treatment.
To establish the grade of kidney cancer, the pathologist examines a sample of tissue taken from the tumor under a microscope. It checks how much cancer cells differ from normal cells (differentiation) and from other characteristics of the tumor such as the size and shape of cells and their arrangement. He can usually tell how fast the tumor is growing by looking at the number of dividing cells.
The pathologist assigns a grade of 1 to 4 (often referred to as a Fuhrman grade) for kidney cancer. The lower this number, the lower the rank.
Low-grade cancers are made up of well-differentiated cancer cells. These cells are abnormal, but they look a lot like normal cells and are arranged very similarly to normal cells. Low-grade cancers tend to grow slowly and are less likely to spread.
High-grade cancers are made up of poorly differentiated or undifferentiated cancer cells. These cells do not look like normal cells and are arranged very differently. High grade cancers tend to grow quickly and are more likely to spread than low grade cancers.
Stages of kidney cancer
Staging describes or categorizes cancer based on how much cancer is in the body and where it was initially diagnosed. This is often referred to as the extent of cancer. Information from tests is used to find out how big the tumor is, what parts of the organ have cancer, if the cancer has spread from where it started and where it has spread. Your healthcare team uses the stage to plan your treatment and predict the outcome (your prognosis).
The most commonly used staging system for kidney cancer is the TNM staging system. In the case of kidney cancer, there are 4 stages. For stages 1 to 4, the Roman numerals I, II, III and IV are often used. But in order to make the text clearer, we will use the Arabic numerals 1, 2, 3 and 4. In general, the higher the stage number, the more cancer has spread. Talk to your doctor if you have questions about staging.
When doctors describe the stage, they can use the words local, regional, or distant. Local means the cancer is only in the kidney and has not spread to other parts of the body. Regional means near or around the kidney. Distant means in a part of the body farther from the kidney.
Stage 1
The tumor is in the kidney and is no more than 7 cm (2,75 inches) in size.
Stage 2
The tumor is in the kidney and measures over 7 cm (2,75 inches).
Stage 3
The tumor has grown outside the kidney and into nearby veins or the layer of fat around the kidney (perirenal tissue). But it did not invade the adrenal gland above the kidney or the fine fibrous tissue that covers the outside of the kidney (Gerota fascia).
OR
The cancer has spread to nearby lymph nodes.
Stage 4
The tumor has passed through the fine fibrous tissue that covers the outside of the kidney and may have grown into the adrenal gland above the kidney.
OR
The cancer has spread to other parts of the body (distant metastasis), such as the lungs, liver or bones. It is also called metastatic kidney cancer.
Kidney cancer recurrence
Recurrence of kidney cancer means that the cancer comes back after treatment. If it reappears where it first started, it is called a local recurrence. If it reappears in tissues or lymph nodes near where it first started, it is called a regional recurrence. It can also reappear in another part of the body: this is called a recurrence or distant metastasis.
If kidney cancer spreads
Cancer cells can spread from the kidney to other parts of the body. This spread is called metastasis.
Understanding how a type of cancer usually grows and spreads helps your healthcare team plan your treatment and future care. If kidney cancer spreads, it can spread to the following parts of the body:
- lymph nodes around the kidney
- main vein of the kidney (renal vein)
- large vein in the abdomen that leads to the heart (vena cava)
- adrenal glands
- other kidney
- lungs
- liver
- bone
- brain
Prognosis and survival for kidney cancer
If you have kidney cancer, you may be wondering about your prognosis. A prognosis is the act by which the doctor best assesses how cancer will affect a person and how they will respond to treatment. The prognosis and survival depend on many factors. Only a doctor who is familiar with your medical history, the type of cancer you have, the stage and other characteristics of the disease, the treatments chosen and the response to treatment can review all of this data together with survival statistics. to arrive at a prognosis.
A prognostic factor is an aspect of cancer that a doctor takes into account when making a prognosis. A predictor factor influences how cancer responds to a certain treatment. We often discuss prognostic and predictive factors together. They both play a role in choosing the treatment plan and in establishing the prognosis.
The following are the prognostic factors and predictors of kidney cancer.
Stadium
The most important prognostic factor is the stage of kidney cancer. A person whose tumor is confined to the kidney has a better prognosis than a person whose cancer has spread outside the kidney.
Grade
A low-grade tumor has a better prognosis than a high-grade tumor. The low-grade tumor is less likely to spread because it grows slowly. The high-grade tumor is more aggressive and tends to spread quickly.
Type of kidney cancer
Papillary or chromophobic renal cell carcinomas have a better prognosis since they are often low grade.
Collector tube carcinoma and bone marrow carcinoma have a poor prognosis since they are often very aggressive.
Risk level
The most common system used to predict the prognosis of people with metastatic renal cell carcinoma is the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC). It is made up of the following 6 predictors:
The Karnofsky Functional Index is below 80.
Less than 1 year has elapsed between diagnosis and treatment of metastatic cancer.
The level of calcium in the blood is abnormally high.
The number of red blood cells is lower than normal (anemia).
The number of platelets is higher than normal (thrombocytosis).
The neutrophil count is abnormally high (neutrophilia).
We combine these predictors to form a risk level:
- Favorable risk means that the person does not have any of the predictors.
- Medium risk means that the person has 1 or 2 predictors.
- A bad risk means that the person has at least 3 predictors.
Treatments for kidney cancer
If you have kidney cancer, your healthcare team will make a treatment plan just for you. It will be based on your health and specific cancer information. When your healthcare team decides which treatments to offer you, they take the following into consideration:
- the stage of kidney cancer
- only one or both functional kidneys
- the presence of cancer in only one or both kidneys
- the type of kidney cancer
- your overall health
You may be offered the following treatments for kidney cancer.
Surgery
Surgery is the main treatment for kidney cancer. It is used to remove part or all of the kidney. This operation is called a nephrectomy. The type of nephrectomy you will have depends on the size of the tumor, its location in the kidney, and the stage of the cancer. Doctors do a partial nephrectomy when possible to leave part of the kidney in place. In some cases, they have to do a radical nephrectomy, which involves removing the entire kidney, in an attempt to completely remove the tumor from the kidney.
Surgery may also be used to relieve pain or reduce symptoms of advanced kidney cancer. It is palliative surgery.
Targeted therapy
In targeted therapy, drugs are used to target specific molecules, such as proteins, on the surface or inside of cancer cells. By targeting these molecules, drugs stop the growth and spread of cancer cells while limiting damage to normal cells. The type of targeted therapy used depends on the type of kidney cancer, the level of risk, and any targeted drugs that have been given to you.
Targeted therapy is used to treat kidney cancer that cannot be completely removed with surgery because it is too advanced. This includes cancer that has spread to other parts of the body and kidney cancer that comes back after being treated.
Ablation
Ablation uses heat or cold to destroy the tumor in the kidney. It destroys kidney cancer cells while preserving as much surrounding kidney tissue as possible. There are two types of ablation that are used to treat kidney cancer. Radiofrequency ablation uses heat. Cryoablation uses cold.
It can be offered to people who cannot have surgery or who need to keep as much of their kidney as possible.
Arterial embolization
The kidney tumor needs blood to grow. Arterial embolization blocks the blood supply to the tumor, which helps to reduce its size. It can be used before surgery to reduce the bleeding if a large tumor is removed from the kidney. Arterial embolization can also be used to relieve pain when a person with advanced kidney cancer cannot have surgery.
Radiotherapy
In external beam radiation therapy, a device that is outside the body is used to direct radiation to the tumor and surrounding tissue. It is usually not given to the kidney tumor itself, but rather to the areas where the cancer has spread, especially to the bones and the brain.
Radiation therapy is also used to relieve pain or control symptoms of advanced kidney cancer.
Immunotherapy
Immunotherapy uses the immune system to help destroy cancer cells. Cancer, and some of its treatments, can weaken the immune system. Sometimes the immune system doesn’t recognize that cancer cells are different, so it doesn’t try to destroy them. Immunotherapy stimulates the immune system to help it recognize and fight cancer cells.
There are 2 types of immunotherapeutic drugs used in Canada, namely immune checkpoint inhibitors and cytokines. Cytokines are not usually used in Canada because the targeted drugs are more effective in treating kidney cancer. But they can be given in specialized treatment centers where immunotherapy has been administered for a long time.
Find out more about immunotherapy.
Active surveillance
If you have kidney cancer but have not had any symptoms, you may be offered active surveillance. This means that your healthcare team is watching the cancer carefully rather than treating it right away. Treatment is given when symptoms appear or when the cancer changes.
You may be offered active surveillance if you have a serious medical condition that makes you unable to tolerate treatment or if the kidney tumor is less than 4 cm (1.5 in).
If you cannot or do not want to be treated for cancer
You may want to consider care that aims to make you feel better without treating the cancer itself, perhaps because cancer treatments no longer work, or they are no longer likely to improve your condition, or cause them to work. secondary are difficult to tolerate. There may be other reasons why you cannot or do not want to be treated for cancer.
Talk to members of your healthcare team. They can help you choose advanced cancer care and treatment.
Monitoring
Follow-up after treatment is an important part of caring for people with cancer. You will need to have regular follow-up visits, especially during the first 3 years after treatment. These visits allow the healthcare team to monitor your progress and to know how you are recovering from treatment.
Clinical tests
Ask your doctor if there are clinical trials underway in your country for people with kidney cancer. Clinical trials aim to find new methods of preventing, detecting and treating cancer.
Active surveillance for kidney cancer
If you have kidney cancer but have no symptoms, you may be offered active surveillance. This means that your healthcare team is watching the cancer carefully rather than treating it right away. She will do tests and check you to see if kidney cancer is growing or spreading. Treatment is given when symptoms appear or when the cancer changes.
This approach helps to avoid the problems or side effects that can occur when using treatments such as surgery or targeted therapy. To date, there is no evidence that people with kidney cancer will not live as long if active surveillance is used instead of other treatments. And there is also no evidence that active surveillance causes any other negative effects if or when you start treatment.
You may be offered active surveillance if:
- you are elderly or have a serious medical condition which makes you unable to tolerate the treatment;
- the cancerous tumor in the kidney is less than 4 cm (1.5 in);
- the cancer has spread to other parts of your body and you are having few or no symptoms at all.
Follow-up after treatment for kidney cancer
Follow-up after treatment for kidney cancer is an important part of the care you receive. Cancer specialists (oncologists), the urologist and your family doctor often share this responsibility. Your healthcare team will talk to you to decide which follow-up meets your needs.
Don’t wait until your next scheduled appointment to report any new symptoms and any symptoms that don’t go away. Tell your healthcare team if you have the following:
- headache
- memory changes
- cough that does not go away
The risk of kidney cancer coming back (coming back) is greatest within 3 years after treatment, so you will need close monitoring during this time. Kidney cancer can come back long after treatment is finished, so it is important to continue to see your healthcare team regularly.
Planning of follow-up visits
Follow-up visits for kidney cancer are usually scheduled for the first 6 years after treatment:
- every 3 to 6 months after initial treatment for 3 years;
- then once a year after 3 years.
Progress of follow-up visits
During a follow-up visit, your healthcare team will usually ask you questions about the side effects of treatment and your ability to cope. She can also learn about your diet and lifestyle.
Your doctor may do a physical exam including:
- feel your abdomen, side and lower back;
- observe your surgical scar to see if it is healing well or if it has changed.
Examinations are often ordered as part of the follow-up. We could ask these:
kidney function blood tests to make sure the remaining kidney is healthy
liver function blood tests to see if there are any problems with the liver that could mean that the cancer has come back in the liver
ultrasound of the abdomen to look at the remaining kidney to make sure it is healthy and functioning
CT scan to look at the remaining kidney and look for changes in the abdomen, including the liver
chest x-ray to see if cancer has come back in the lungs
You may need to have follow-up tests more often if your risk of recurrence is medium or high because the tumor is large, the cancer has spread to the lymph nodes, or both.
If your healthcare team finds out that the cancer has come back, they will talk to you to plan your treatment and care.
Supportive care for kidney cancer
Supportive care empowers people to overcome the physical, practical, emotional and spiritual barriers of kidney cancer. It is an important component of the care of people with this disease. There are many programs and services that meet the needs and improve the quality of life of these people and their loved ones, especially after treatment is over.
Recovering from kidney cancer and adjusting to life after treatment is different for everyone, depending on the stage of the cancer, the type of treatment, and many other factors. The end of cancer treatment can lead to mixed emotions. Even if treatment is finished, there may be other issues to work out, such as coping with long-term side effects. A person who has been treated for kidney cancer may be concerned about the following.
Living with just one kidney
You can lead a normal, healthy life with only one functioning kidney or with only part of a kidney. The rest of the kidney tissue is still able to filter waste and excess water from the blood.
It is important that you take care of the remaining kidney. You can help your kidney function properly by following the tips below.
Quit smoking
Smoking is the biggest risk for kidney cancer. It also increases the risk of kidney cancer coming back. If you smoke, get help to quit.
Talk to a dietitian about your diet
When the kidney that remains is healthy, you usually don’t have to change your diet. If the kidney that remains is not completely healthy, or if only part of the kidney is left, talk to a dietitian about changes you can make to your diet.
Try to eat less protein, such as meat, fish, eggs, milk and dairy products, and beans. Consuming too much protein causes stress on the kidney.
Reduce the amount of salt you eat. Avoid eating pretzels, chips, popcorn, and processed canned meat, poultry, and fish. Do not add salt to your food and limit the number of times you eat restaurant prepared food. The kidneys filter salt from the blood, so if the food you eat contains a lot of salt, the remaining kidney has to work harder.
Limit the amount of phosphorus you consume. When your kidneys are not working well, the level of phosphorus in your blood may increase. This can cause problems like joint pain. Your dietitian may recommend that you limit the amount of foods high in phosphorus, such as seeds, nuts, peanut butter, lentils, and beans.
Limit the amount of liquids you swallow, such as water, coffee, tea, soup, gelatin desserts, and ice cream. Staying well hydrated is important, but drinking too much fluid can be stressful on your kidneys.
Limit the amount of alcohol you drink. Drinking a lot of alcohol can damage the kidneys. If you decide to drink alcohol, do not take more than 1 drink per day.
Dialysis
When the kidneys are not working properly (renal failure), dialysis must be used to remove waste products from the blood. Kidney failure can be a short- or long-term side effect of treatments for kidney cancer. In rare cases, a person may need dialysis for the rest of their life if both kidneys have been removed or their only functioning kidney has been removed.
Hemodialysis
In hemodialysis, a device is used to filter waste and excess water from the blood. A special tube, called a dialysis catheter, is inserted into a large vein in your body. Small amounts of blood are removed from your body, the device filters it, and then it is returned to your body.
You will be dialysis 3 times a week. You will be hooked up to the machine for a certain number of hours each time you hemodialysis. If you need to be on dialysis for the rest of your life, a surgeon will provide permanent access to your bloodstream during surgery.
Peritoneal dialysis
Peritoneal dialysis uses the membrane that surrounds the organs in your abdominal cavity (peritoneum). The most common type of peritoneal dialysis is called continuous ambulatory peritoneal dialysis (CAPD).
The doctor inserts a tube (catheter) into the muscles in your abdomen. This tube remains in place permanently. During dialysis, the healthcare team attaches bags filled with a special dialysis solution to the tube. This solution circulates in your abdomen. The peritoneum allows waste and excess fluid to pass from the blood to dialysis solution. The dialysis solution stays in your abdomen for many hours, absorbing the waste. The solution is then drained and replaced with a fresh solution.
The advantage of peritoneal dialysis is that it can be done at home, allowing you to continue with your daily activities.
Diet during dialysis
A dietitian may recommend that you eat in a special way to stay healthy while on dialysis:
restrict the amount of fluids you swallow;
opt for a diet rich in protein (since you lose protein during dialysis);
reduce the amount of salt, potassium and phosphorus you eat.
List of all Cancers
The word “cancer” is a generic term for a large group of diseases that can affect any part of the body. We also speak of malignant tumors or neoplasms. One of the hallmarks of cancer is the rapid multiplication of abnormal growing cells, which can invade nearby parts of the body and then migrate to other organs. This is called metastasis, which is the main cause of death from cancer. Types of cancer (in alphabetical order of the area concerned):
Information: Cleverly Smart is not a substitute for a doctor. Always consult a doctor to treat your health condition.
Sources: PinterPandai, American Cancer Society, Web MD, Cancer Center, Cleveland Clinic
Photo credit: Wikimedia Commons